What is it?
This is a frightening name for a common condition. There is much variation and some confusion with how this word is used. The following is a brief outline:
Scheuermann’s Kyphosis
A Danish radiologist (specialist who interprets x-rays) in the 1920s wrote an article describing the x-ray changes in a condition described as juvenile kyphosis. Kyphosis is further explained below, but refers to an excessive forward bend of the upper (thoracic) spine. The condition of kyphosis in a teenager where there are the x-ray changes that he described is called “Scheuermann’s kyphosis”. This is what most spinal surgeons mean by Scheuermann’s disease.
Changes of Scheuermann’s Disease on X-Ray
Some of the x-ray findings that were originally described may be seen on x-rays of the spine, even without the spinal deformity of kyphosis being present. This is what most radiologists mean by Scheuermann’s disease.
What is kyphosis?
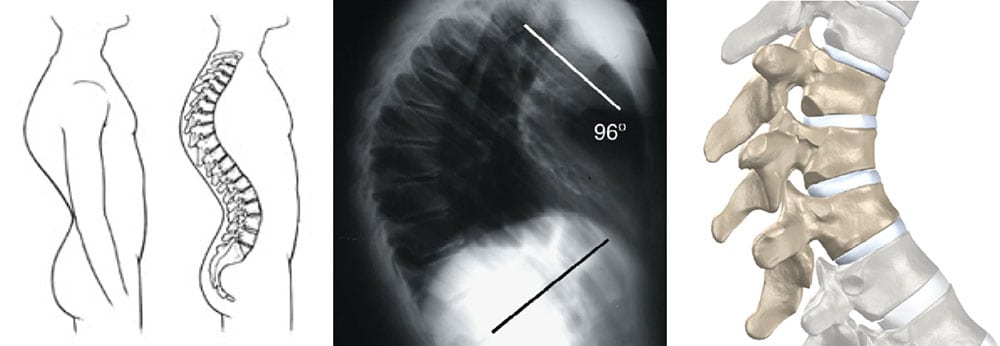
This is a forward bend in the spine. Everyone’s spine has a kyphosis or forward bend in the upper back (thoracic spine). It is normal, and is part of the S-shape of the normal spine. The kyphosis may be excessive, and this is what doctors mean when they say ‘you have a kyphosis’. The normal angle is 20° to 40°, and it is considered abnormal if it is more than 45°. An increased kyphosis is sometimes called ’roundback’ or ‘hunchback’. There are a number of causes. The most common is probably postural. This is due to slouching and poor posture, but if prompted, the person can straighten the spine if they want. This usually goes away after teenage years and is not important in the long term. The other type is structural, where the shape cannot be corrected if the person tries to stand up straight. There is an underlying abnormal shape of the vertebra. By far the most common of these is Scheuermann’s kyphosis. Other causes include a birth defect where the vertebrae have not formed properly, or after a spinal fracture. In older adults (especially elderly women), kyphosis can also occur, but it is due to weakening and collapse of the bones from osteoporosis. This is a different condition.
What is the cause of Scheuermann’s Disease?
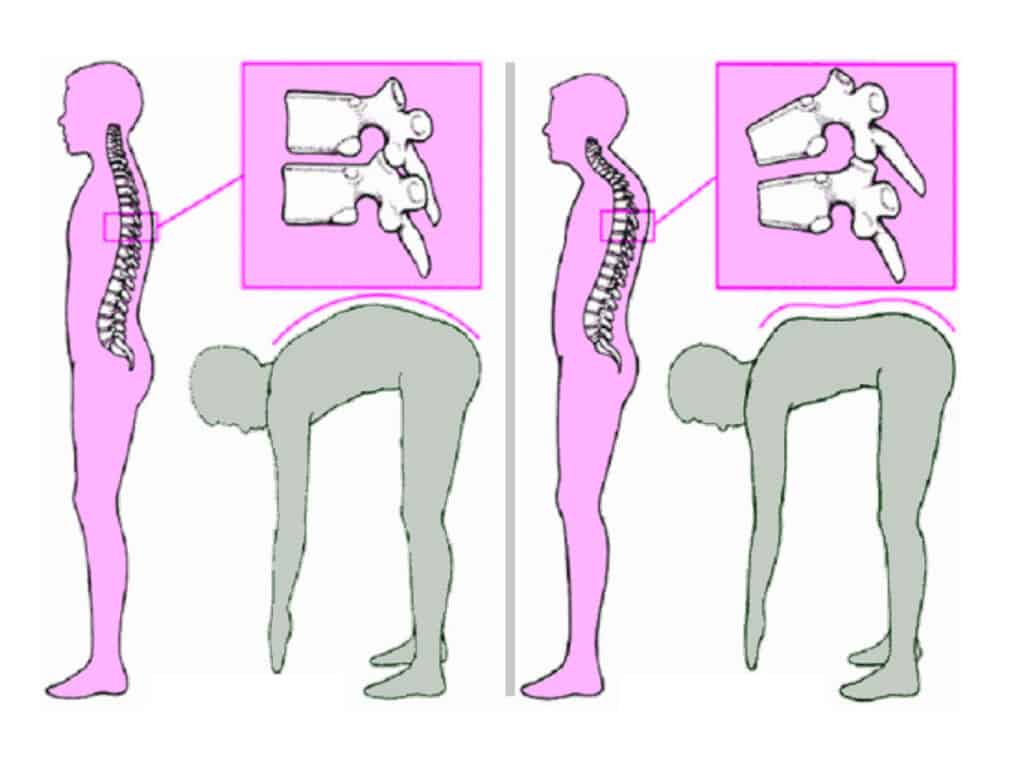
The simple answer is – nobody knows for sure. The problem is with the vertebral end-plates – the upper and lower surfaces where growth of the vertebra occurs. The abnormal growth here may be due to a pre-existing weakness with the cartilage and bone here, or due to excessive force on the bone. It is probably a combination of both. There is a slightly increased incidence in some families. This does not mean that if you have it, you will definitely pass it on to your children, but that there may be a very small increase in the chance that they may have some of the changes.
What are the x-ray changes of Scheuermann’s Disease?
There are a number of changes seen. Strictly to be classed as Scheuermann’s kyphosis, there must be wedging of vertebrae, where they are smaller at the front than at the back. As you can imagine, if a number of adjacent vertebrae are wedged at the front, a curve will occur. This is the main cause for the kyphosis. As well, there is end-plate irregularity, where the upper and lower surfaces of the vertebrae are not smooth. Instead they are uneven. Another finding is disc space narrowing where the space on x-ray between the vertebrae (where the disc is found) is decreased. The final finding is Schmorl’s nodes, which are rounded ‘divots’ or defects in the vertebral end-plate. The most common area of the spine to see these x-ray changes is in the mid-thoracic spine but they can less commonly be found in the lower thoracic or upper lumbar spine. This is sometimes referred to as the thoracolumbar variant of Scheuermann’s disease.
How common is Scheuermann’s Disease?
It depends on what is meant by Scheuermann’s disease. In a study of children between 17 and 18 years old, the x-ray changes were present in more than 50% of boys and in 30% of girls. In other words, if an x-ray report mentions Scheuermann’s disease, it really doesn’t mean much, as it is common enough almost to be considered normal. On the other hand, true Scheuermann’s kyphosis is much less common, and is present in about 1% of people. It appears to be a little more common in boys than girls.
What does it cause?
It is important to note that most people with x-ray changes of Scheuermann’s disease do not have any symptoms. Even those with a kyphosis often have no discomfort.
Altered Shape
The increased kyphosis (roundback) is the most common thing people notice. The curve in the upper back is usually sharp rather than smooth, and stiff rather than flexible, which differentiates it from poor posture. To compensate for the curve, there is usually an increased lordosis in the low back or lumbar spine (sometimes called a swayback). Depending on the person’s body shape, the kyphosis may be more or less noticeable, and worries some people more than others. The curve can increase in size while the spine is growing.
Pain
There may be an ache in the region of the curve, which is often worse after physical activity. The degree of pain varies from one person to another, but is almost never incapacitating. It is thought that there is more chance of significant pain in the thoracolumbar variant (where the condition involves the lower thoracic and upper lumbar spine rather than the midthoracic spine).
Other
It is almost unheard of for it to cause any weakness in the legs or paralysis. The curve has to be very large before there is a possibility of this.
What happens in the future?
This is not clear. The most common age for people to come to the doctor with this condition is as a teenager or young adult. This is usually when symptoms are first noticed. Doctors do not often see older adults coming along for the first time. This may be because most people make some adjustments and are able to lead relatively normal lives. It also may be that the pain decreases with age. One study suggested that most people with the condition ended up not doing heavy physical jobs, but were able to lead normal working lives. There is a suggestion that the normal degenerative changes seen on x-ray in the spine occur earlier in people with Scheuermann’s disease, but it has not been shown to cause increased back pain in later years. Unless it is very large, the curve stops increasing in size when the spine stops growing (by age 18).
What can be done?
Of course, if there are no symptoms, nothing need be done.
Exercise and Physiotherapy
Back strengthening and stretching can be useful to decrease stiffness in the spine. A physiotherapist can help design an exercise programme. Activities such as swimming may be beneficial. You must remember that none of these will decrease the kyphosis. They may maintain some flexibility and decrease the pain but will not alter the progression of the condition.
Medications
Simple pain killers such as aspirin or paracetamol may help cope with flares of pain. Anti-inflammatories may also be used but they act more like pain killers as there is no true inflammation associated with the condition.
Observation
If there is a curve and the spine is growing (i.e., before age 18 or so) the curve is watched every six to twelve months, and x-rays are usually repeated. Once it is clear the curve is small and not progressing or the spine has stopped growing, there is usually no further need to keep checking the spine.
Bracing
A brace may sometimes be prescribed by your doctor. It works by pushing the spine straight and encouraging the vertebrae to grow more evenly. It is a cumbersome thing and must be worn continuously until about age 17. For a teenager, this can be fairly drastic. It is used when the curve is big enough to justify it (usually greater than 60°) and when the spine has some growth left (often no older than age 14). It does not correct the spine completely but often makes a reasonable improvement. The decision if and when to use a brace is complex and the pros and cons cannot be adequately explained here.
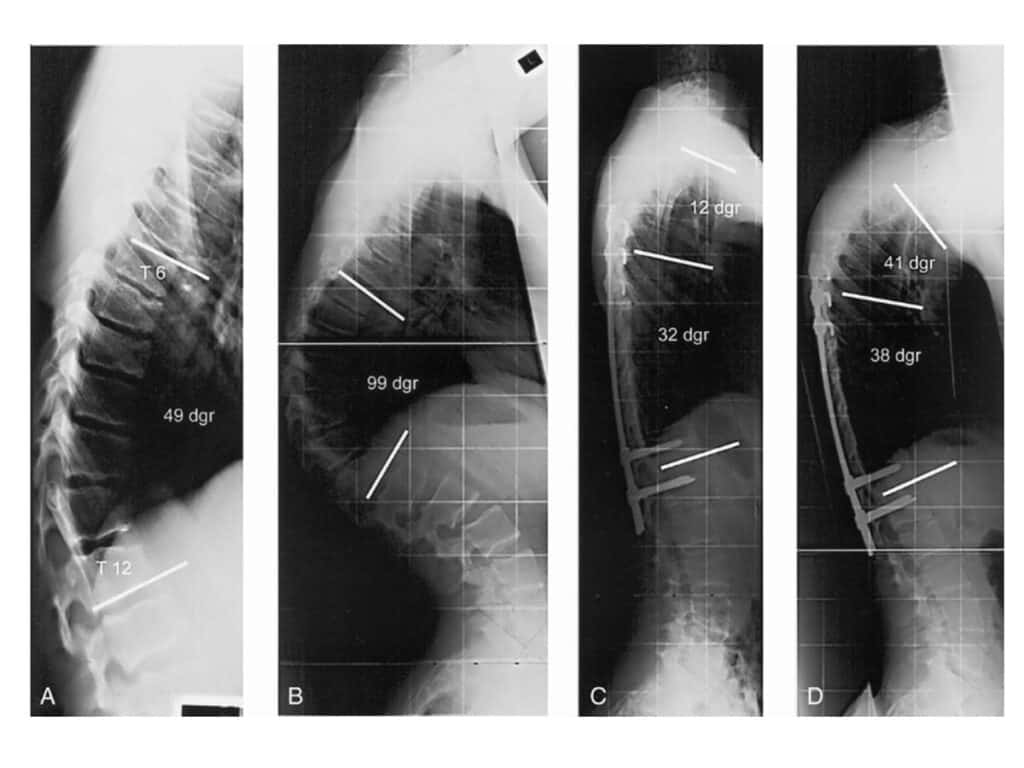
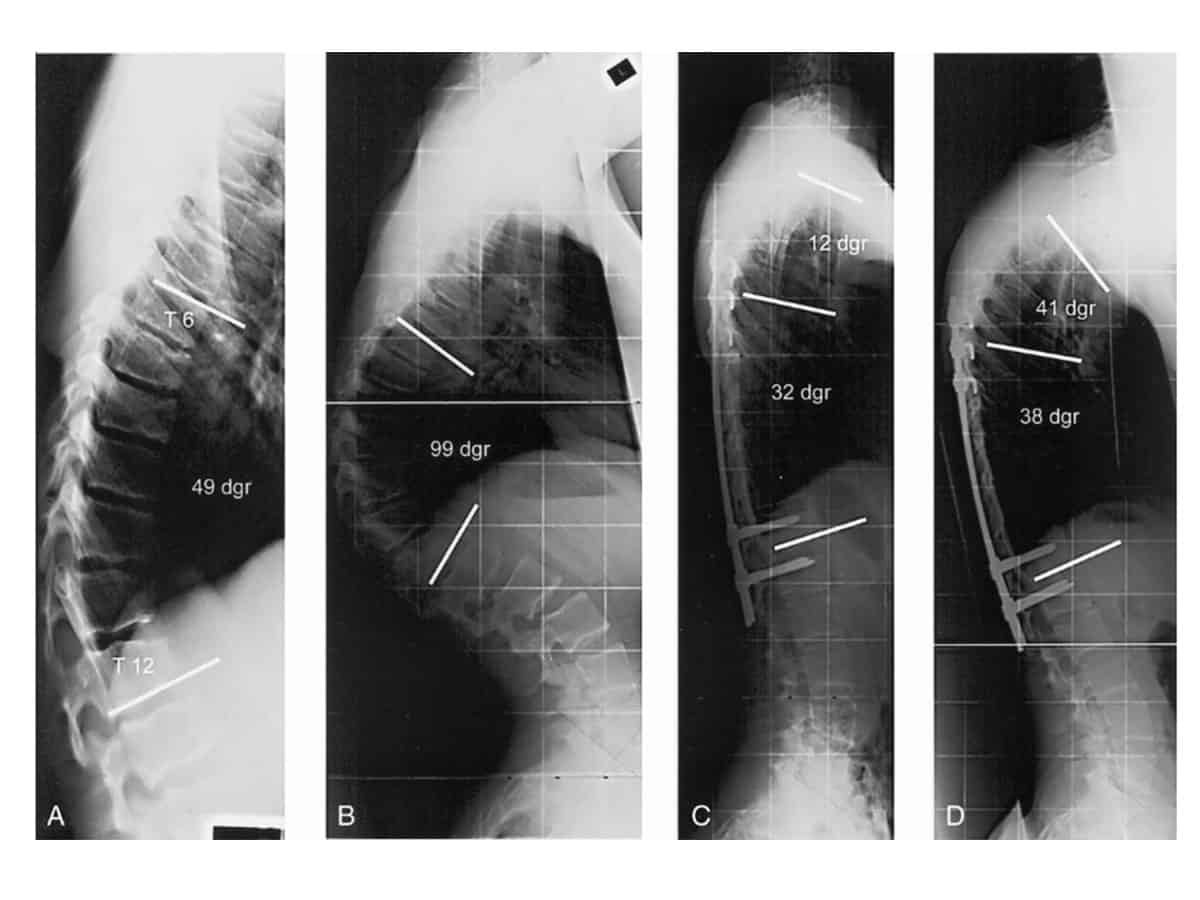
Surgery
This may be used for very large curves (usually greater than 70°) if the curve is very painful or cosmetically unacceptable, and a brace has either been unsuccessful or is not suitable. If the curve is very stiff, an operation from the front of the spine through the chest needs to be done to release the spine and improve the chances of correction. The main part of the operation is the correction from the back of the spine. Rods are inserted to pull the spine straight and hold it there, and a fusion is done to join the bones together to keep the spine straight. It is a complex operation and there are risks of paralysis, of the rods pulling out and of infection. For these reasons, it is not done very often and the decision needs to be made very carefully.